Download and print as a PDF
DownloadUrethrolysis an operation carried out to correct obstruction to passing urine after surgery for stress incontinence of urine (leakage of urine on coughing and sneezing).
The operation aims to free the urethra, so that urine can flow out easily. It can be done vaginally, abdominally (through a cut across the tummy) or laparoscopically (through key hole surgery).
Vaginal and abdominal operations can be carried out under general or spinal anaesthesia. The laparoscopic approach requires general anaesthesia.
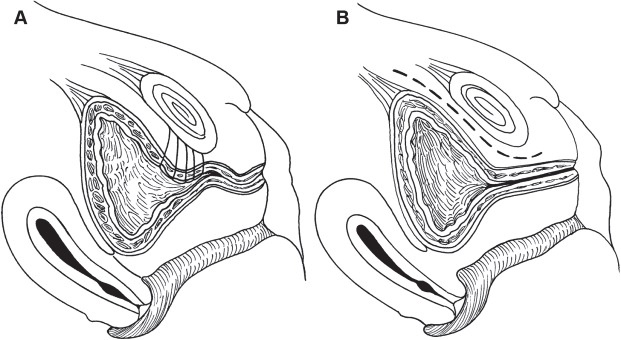
Freeing the urethra during urethrolysis.
The operation is intended to improve passing urine. This will help you with problems caused by difficulty in emptying the bladder, like dribbling at the end of passing urine, pain, repeat and / or urgent need to pass urine, urinary leakage and repeat urinary tract infections.
At your pre operative assessment and on your admission day, the nurse will go through your hospital stay and explain your operation. Please do let us know about any concerns you have, or if there is any information you think we should know, that will make your stay with us more comfortable.
Before coming into hospital you will need to make alternative arrangements for any caring or other responsibilities that you have during your admission and your recovery period at home.
You will see an anaesthetist and the doctor performing the surgery before you go to theatre. It is not unusual to feel anxious; the nursing staff will gladly discuss with you how you are feeling and talk you through your emotions.
If you have not already signed the consent form, the doctor will go through it with you before you go to theatre.
You will be asked for permission to enter your data on the national database for continence and prolapse surgery. This is a quality control measure to compare the safety and effectiveness of such procedures at the hospital against other units in the country.
If you have not already completed a quality of life questionnaire, you will be asked to do so before surgery.
You will be given a copy to complete and bring with you when you attend your follow up appointment after surgery. This will assessing the benefit of surgery for you.
If the operation is to be done vaginally, it will entail a cut inside the vagina.
If the operation is to be done abdominally, it will entail a cut through the tummy wall. This cut is usually across the tummy, but it might have to be vertical (up/down).
If the operation is to be done laparoscopically, it will entail three small cuts across the tummy. One of these cuts is made in the umbilicus (belly button). In patients who had previous surgery with open cuts across the tummy, this cut may have to be below the chest wall (rib cage) on the left side. The other two cuts are lower down on either side.
Regardless of the route, the urethra will be mobilised from its fixed position, to have more mobility. The cuts made will then be closed, with dissolvable stitches.
The choice between the three approaches will depend on the operation(s) you had before and whether key hole surgery is possible or not. This will be discussed with you before any planned is agreed with you.
There are risks with any operation but these are small.
The main risks associated with a urethrolysis are:
Common risks:
Uncommon risks:
In order for you to make an informed choice about your surgery please ask one of the doctors or nurses if you have any questions about the operation before signing the consent form. What are the risks?
As you come round from the anaesthetic, you may experience episodes of pain or nausea. Please let the nursing staff know and they will assess you and take appropriate action.
A small drain may be placed in the abdominal wound to remove any excess blood.
A catheter might be inserted to drain the bladder. This will save you having to go to the toilet, till you are fully mobile after the operation.
You may have a drip to give you fluids, though you will be able to eat and drink normally.
You may have a Patient Controlled Analgesia (PCA pump) to control your pain. This is not common and will be discussed with you before the operation by the anaesthetist.
The nurses will assess you regularly to ensure that the PCA is effective. We will use a pain score to assess your pain 0 to 10; 0 No Pain, 10 Very Strong Pain.
Your nurse will be checking your blood pressure, pulse, breathing, temperature, monitoring the wound across your abdomen and checking for any vaginal bleeding. S/he will also ask you to move from side to side and to do leg and breathing exercises. This will help prevent any pressure damage, blood clots in legs or lungs or chest infection.
The first 12 hours after the operation
You can expect pain and discomfort in your lower abdomen for the first few days after the operation and will be given pain killers to help control this.
Day 1 after the operation
The drain, drip and catheter that drains the bladder are usually removed the next day.
The nursing staff will assist with washing as necessary and encourage early mobilisation. We would normally expect you to sit out of bed and begin to walk around the day after your operation.
You will be able to go home when you are passing urine without difficulty. You will be asked to pass urine in a jug and will have a scan to measure how much urine is left in the bladder. It is advisable to forget that you need to pass urine and drink and walk as you would normally do. This helps your bladder to work as normal.
You will have a dressing on the wound across your abdomen that will be removed the day after your operation and you will be able to shower.
You may also find it difficult to open your bowels at first, you will be given mild laxatives to soften your stools and prevent constipation and straining.
You will be seen and assessed by the Gynaecology team the following day to check on your recovery and decisions will be made about your care, this information will be shared with you. You may then be able to go home. Please feel free to ask questions about your operation and recovery at any time.
The average length of stay following urethrolysis is 1 to 2 days. In most instances you can go home the following day. As you physically recover from your operation, the nursing team will discuss your convalescence. To ensure you have a good recovery you should take note of the following:
Rest:
During the first two weeks at home it is common to feel tired and emotional. You should relax during the day gradually increasing the number of things you do each day. Avoid crossing your legs when you are lying down.
Vaginal bleeding:
You might have some vaginal discharge or bleeding for few days after surgery. This should be very slight and you should use a sanitary towel. Tampons should not be used to reduce the risk of infection.
Stitches:
The wound(s) across your abdomen will be closed by dissolvable stitches. If after 7 days you notice the stitches have not dissolved then they will need to be removed. This is normally done by your practice nurse and you will need to make an appointment.
Showering:
We advise that you shower daily and keep the abdominal (tummy) wound(s) clean and dry. There is no need to cover the wound with a dressing.
Housework:
Weeks 1 to 2: We recommend that you do light activities around the house and avoid any heavy lifting (not more than 1.5kgs in each hand).
Weeks 3 to 4: We recommend that you gradually introduce lighter household chores, dusting, washing up, making beds and ironing. You may begin to prepare food and cook remembering not to lift any heavy items.
Weeks 4 to 6: By this time you should resume normal daily activities, but continue to refrain from straining until 3 months after surgery, to ensure good healing of the sling.
Exercise:
Exercise is important and it is advisable to go for short walks each day, increasing the distance gradually. You will be able to manage the stairs on your arrival home. We encourage you to do pelvic floor exercises.
You should avoid straining or heavy exercise for 3 months, to ensure good healing of the sling. You may return to normal exercise such as cycling and swimming after 4 to 6 weeks. You will be given a physiotherapy booklet titled ‘Fit for Life’ to guide you.
Diet:
A well balanced nutritious diet with high fibre content is essential to avoid constipation. Your bowels may take some time to return to normal after your operation and you may need to take laxatives. You should include at least 5 portions of fruit and vegetables per day. You should aim to drink at least 2 litres of water per day.
Sex:
You should usually allow 4 to 6 weeks after the operation before having sex to allow the vagina to heal.
If you experience vaginal dryness, you may wish to try a vaginal lubricant from your local pharmacy.
If after this time you are experiencing pain or any problems with intercourse then you should see your GP.
Returning to work:
This will depend on the nature of your work. If you work in an office base environment, you will need 4 to 6 weeks off work. If your work involves lifting and exertion, you will need 3 months off work. The hospital doctor will provide a medical certificate for this period.
Driving:
It is usually safe to drive after 12 weeks. This will depend on your level of concentration and ability to perform an emergency stop. It is advisable to check with your insurance company.
You will be invited for follow up, usually at Lewes Victoria Hospital about 12 weeks after surgery. During this follow up appointment, your symptoms will be reviewed and you will be examined to assess wound healing.
If you have problems before this you can either contact your doctor or contact the hospital to bring the appointment forwards.
You have been counselled about, and probably tried, intermittent self catheterisation before urethrolysis was considered. You may have tried medication for overactive bladder and / or antibiotics for urinary tract infections.
You should contact your GP or the hospital if you notice:
If you have any problems or questions, you can contact:
The Urogynaecology Unit at Lewes Victoria Hospitalon 01273 474 153 Extension 2178
The Gynaecology Ward at the Princess Royal Hospital on 01444 441 881 Extension 5686
The Gynaecology Ward at the Royal Sussex County Hospital on 01273 696 955 Extension 4013
References and useful links:
If you do not understand this leaflet, we can arrange for an interpreter.
This information leaflet has been produced by Dr. Sharif Ismail, Consultant Subspecialist Urogynaecologist.
This information leaflet has been approved at the Clinical Governance and Safety and Quality Meetings of the Department of Obstetrics and Gynaecology as well as Brighton and Sussex University Hospitals NHS Trust Carer and Patient Information Group (CPIG).
This information is intended for patients receiving treatment at Brighton or Haywards Heath.
This information is for guidance purposes only and is in no way intended to replace professional clinical advice by a qualified practitioner.
Publication Date: March 2021
Review Date: December 2023
