Download and print as a PDF
DownloadPlease be aware that there are images of wounds on this page
1. Your orthopaedic surgery (fixing the bone)
2. Your plastic surgery (soft tissue reconstruction)
3. What to expect after your surgery
4. Commonly asked questions.
An open fracture is a broken bone that has come through the skin. They are typically caused by high-energy injuries such as road traffic collisions, falls or sports injuries. Urgent treatment is required as open fractures are at much greater risk of infection, and delayed healing of the bone, compared to fractures with intact skin. Bone infection can be difficult to treat and in a worst-case scenario, amputation of the limb might be required, although this is unusual.
As the skin over the fracture has been broken, infection can spread easily to the fracture site. Patients with open fractures require urgent surgery performed by orthopaedic and plastics surgeons working together to remove any debris, clean the wound and remove any unhealthy tissue.
This is known as debridement and often leads to a larger wound in the skin. Debridement is crucial as any dead tissue or bone left in the wound can lead to infection. Antibiotics and a tetanus booster are given at the same time.
After the debridement is complete, and if the wound can be closed (stitched together), the bone can be fixed together internally (internal fixation).
If internal fixation doesn’t work, you will be fixed together externally as a temporary measure (external fixation), and the wound will be covered, usually with a suction dressing (picture below). You will then return to theatre in the next few days for final bone fixation by the orthopaedic surgeon and soft tissue reconstruction by the plastic surgeon in a joint operation.

Suction dressing
You will meet with the Orthopaedic and Plastic Surgery Team before the operation. They will make sure it is safe for you to have surgery and will be happy to answer any questions you may have. The surgeons participating in this operation will be highly trained professionals, who have years of experience and have been involved in a lot of these kind of operations before.
You may also have:
Open fractures almost always need surgery to put the bone back and hold it there while it heals. This can be done in a number of ways. Examples are shown below. Your surgeon will discuss with you what he/she feels is in your best interest.
External fixation is when pins or wires into the bone are attached to rings or rods outside the limb. External fixators are used commonly as a temporary measure but can also be used as the final treatment and removed once the bone has healed.

External fixation of the bone
Internal fixation is when either a rod inside the bone or plates on the surface of the bone are fixed to the bone with screws. These generally stay in forever but can be removed if there are any problems, but this is very uncommon.

Intramedullary nail or rod bony fixation

Plate and screws bony fixation
In an open fracture there can be significant damage to, and loss of, the skin and muscle around the fracture. In order to reduce the risk of infection to the bone and metalwork, the wound must be closed when the bone is fixed. Unless it is a very small hole that can be closed, a soft tissue reconstruction is required. These operations are usually long (can take all day), and a general anaesthetic is most commonly used, unless otherwise advised from the Anaesthetic team.
Depending on the size and location of the wound, as well as the cause, the Plastic Surgery team may use:

Recently healed skin graft donor site on the thigh.
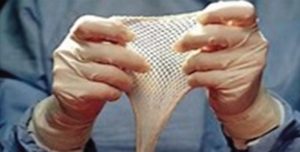
Meshed skin graft.

Skin and fat flap mobilised to cover wound on leg with secondary wound resurfaced with skin graft.
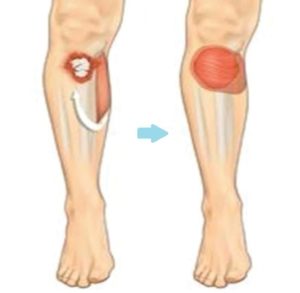
Calf muscle transferred to cover a wound at the front of the leg (picture from www.bapras.org.uk)

Diagram depicts a muscle taken from the thigh to cover a wound over
an open fracture on the other leg; the donor site is closed directly,
and the muscle flap is covered with a skin graft (picture from www.bapras.org.uk).
Soft tissue reconstruction, especially involving muscle, always looks bit bulky at start.
However, as the flap matures over time, its volume reduces. It usually levels with the tissue around it but can sometimes remain a bit bulky.
The colour of the flap changes over time to more or less match the skin next to it. The size and colour change is a process that takes time to settle, usually 9-12 months.
The pictures below show a timeline of a muscle flap immediately after the operation (left), after 3 months (right), and after 9 months (bottom).
Very occasionally, any bulkiness that remains can be treated, if necessary, with secondary procedures.

Muscle flap day 1 after operation

Muscle flap 3 months after the operation.

Muscle flap 6 months after the operation.

A skin and flap day 1 after surgery.

A skin and fat flap 4 months after surgery.
The length of time you are in hospital depends on the extent of the surgery and how quickly you recover. On average, most people stay for seven to 10 days after the surgery.
You should expect some pain after your surgery. The surgical and anaesthetic team will make sure you have all the necessary pain relief prescribed on your drug chart so the nursing staff can provide it. If you are still in pain, please inform your doctor or nurse.
Each person’s pain threshold varies and so does the length of time each person has pain. Please, follow the guidelines below to manage your pain.
The ward physiotherapy will work with you to minimise muscle wastage while an inpatient and the outpatient physiotherapist will follow you after your discharge to work on your mobility and muscle power.
Strong pain medication may cause constipation, but there are steps you can take to prevent it, including exercising if you can. Walking is an excellent form of exercise. Drink plenty of water and make sure you include plenty of fruit and vegetables in your diet. If these methods do not help, talk with your doctor or nurse. He or she may recommend over the counter or prescription medication
We try to use absorbable stitches when we can, however, any non-absorbable stitches will be removed approximately two weeks after your surgery. The stitches may stay in place for longer if deemed necessary from your surgical team.
It is quite important to keep donor site moisturised to improve its cosmetic appearance and avoid ugly scarring, soreness or itching. Details of aftercare and ointment application will be given to you from your surgeons upon discharge.
Your surgeons will give you instructions on when you can shower.
You can swim when you’ve been told that your wounds are completely healed. Avoid hot tubs, baths and swimming pools until then.
This depends on the extent of your surgery and how quickly you recover. On average 80% of patients get back to employment and can expect to get back roughly 75% of their limb function. It is important to realise that it can take a long time to get over an open fracture and that recovery can be on-going up to 18 months after the injury. The fracture may take over six months to heal. Doing exercises and physiotherapy play a key role once your orthopaedic surgeon is happy with the progress of your fracture healing.
You should only return to driving when you are able to perform an emergency stop. On average, this is about six weeks after you are able to fully bear your own weight, but this is different for each person, and their injury.
You may find that you may not be able to play sports as well as before, but able to manage with everyday functions. Do not do strenuous exercise or lift any objects heavier than 2kg for six weeks. Talk with your surgical team before resuming activities such as lifting and exercise.
Your doctor will tell you when you can resume sexual activity.
Both the Orthopaedic and Plastic Surgery teams will need to see you after discharge to monitor the healing of your fracture and soft tissue reconstruction. This is usually done in a joint clinic, (the Orthoplastics Clinic), and/or may be the Plastics Dressings Clinic (PDC). You will be informed of your follow up appointment date and time when you are discharged from hospital.
After surgery for a serious injury, you may have new and upsetting feelings. Many people say they felt weepy, sad, worried, nervous, irritable, or angry at one time or another. You may find that you cannot control some of these feelings. If this happens, it’s a good idea to seek emotional support.
The first step in coping is to talk about how you feel. Family and friends can help. Your nurse, doctor or physiotherapist can reassure, support, and guide you. It is always a good idea to let these professionals know how you, your family, and your friends are feeling emotionally. Many resources are available to patients and their families. Whether you are in the hospital or at home, your nurses and doctors are here to help you and your family and friends handle the emotional aspects of your illness.
If you have any questions or concerns, please contact:
Authors:
Dimitrios Kanakopoulos: Plastic & Reconstructive Trauma Fellow
Andrew Stone: SpR Trauma & Orthopaedics
Enis Guryel: Consultant Trauma & Orthopaedics/Major Trauma Lead
This information is intended for patients receiving care in Brighton & Hove or Haywards Heath.
The information in this leaflet is for guidance purposes only and is in no way intended to replace professional clinical advice by a qualified practitioner
Publication Date: June 2021
Review Date: March 2024
