Download and print as a PDF
DownloadOveractive bladder is a condition characterised by a number of symptoms, including:
The condition can cause considerable distress for patients and affect their quality of life. The fear of having to go to the toilet quickly makes patients look out for toilets all the time. This limits their activity and can lead to withdrawal and isolation. Having to wake up at night to pass urine can lead to disturbed sleep.
Overactive bladder can be a manifestation of other diseases or conditions, such as:
Having an overactive bladder can also be a problem in its own right, without an underlying cause. This happens when there is increased sensation from small volumes of urine in the bladder, with or without causing unwanted bladder contraction (spasm). Habitual frequent passing of urine for fear of leakage can lead to overactive bladder, as a learnt behaviour.
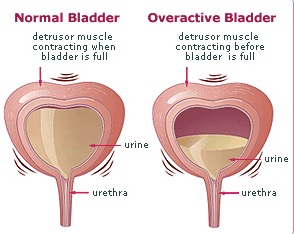
Overactive bladder
Excessive fluid intake, especially coffee, tea, cola and alcohol, as well as smoking, can irritate the bladder enough to cause or worsen the condition.
Overactive bladder can be experienced by patients with pelvic organ prolapse, where loss of support can lead to slipping down of the vagina and / or the uterus.
Overactive bladder may co exist with stress incontinence of urine (leakage of small drops of urine on coughing and sneezing), which is known as mixed incontinence.
It may also follow continence surgery, such as mid urethral tape sling operations and Burch colposuspension.
The diagnosis is helped by completing a frequency volume chart (bladder diary).
An examination is carried out to identify underlying or contributory causes, such as neurological disease, enlarged uterus or pelvic organ prolapse.
Investigations to detect underlying problems include urine dipstick, culture and sensitivity and / or cystoscopy (camera examination of the inside of the bladder).
If underlying or contributory cause(s) can be found, these should be corrected. For example, good control of blood sugar is important in diabetic patients and infection is treated with antibiotics.
If no specific cause can be found, then simple measures are attempted before moving to more complex and invasive lines of treatment.
Fluid advice: For the climate in the UK, a person is expected to drink 24ml / kg / day. This equates to about a litre and half to 2 litres (about 7 mugs or 10 cups) per day.
Bladder training (drill): Trying to hold on for longer periods of time between visits to the toilet may help stretch the bladder. This will enable it to get used to holding larger volumes of urine. The trigger to go to the toilet can be suppressed by tightening the pelvic floor muscles. Patients can be referred for specialist physiotherapy to guide pelvic floor muscle training and bladder drill.
Medication: Tablets are available to reduce overactive bladder. These tablets can be taken once or twice daily. Some have fixed doses whilst the dose of others can be titrated according to response and side effects. A patch is also available. A gel is about to be introduced as well. Common side effects include dry mouth and constipation. The general practitioner will be able to offer one of these medications. It may be necessary to switch medication in the absence of an adequate response and or upon the occurrence of side effects.
These measures are tried for 4 to 6 months. If they don’t work, further tests are carried out.
These tests include:
Modern surgical measures include:
More invasive measures include:
These operations are more invasive and need to be considered carefully due to the potential for complications. They are reserved for extreme cases that do not improve with minimally invasive measures.
Please see below for contact telephone numbers.
Princess Royal Hospital: 01444 441881 Extension 5686
Royal Sussex County Hospital: 01273 696955 Extension 4013
Urogynaecology Unit at Lewes Victoria Hospital: 01273 474153 Extension 2178
Your Pelvic Floor: Overactive bladder
www.patient.co.uk: Overactive bladder
This patient information leaflet was prepared by Dr. Sharif Ismail, Consultant Subspecialist Urogynaecologist.
This information leaflet has been approved at the Clinical Governance and Safety and Quality Meetings of the Department of Obstetrics and Gynaecology as well as Brighton and Sussex University Hospitals NHS Trust Carer and Patient Information Group (CPIG).
This information is intended for patients receiving care in Brighton & Hove or Haywards Heath.
The information here is for guidance purposes only and is in no way intended to replace professional clinical advice by a qualified practitioner.
Publication Date: May 2021
Review Date: February 2024
